Gradial
Gradial  PEGA
PEGA Your pharma stack has a data problem. Here’s what a connected architecture actually looks like.
Jun 17, 2026 | 8 min read
Most pharma organizations don’t have a data problem in the way they think they do. The data exists. It’s in the CRM, the claims systems, the hub platforms, the enrollment tools, and the market access databases. The problem is that none of it connects into something the business can act on. A connected Salesforce architecture, built on Life Sciences Cloud, Data Cloud, and MuleSoft, changes that. But only when the operating model, data model, and integration strategy come before the technology decisions.
Walk into most mid-to-large pharma organizations and you’ll find the same setup. The CRM holds field engagement history. A separate system manages patient enrollment. Another tracks market access and payer data. A fourth handles HCP affiliations and NPI records. And a reporting layer tries to connect all of it. It doesn’t really work. Decisions still get made on gut instinct, outdated exports, and manual reconciliation.
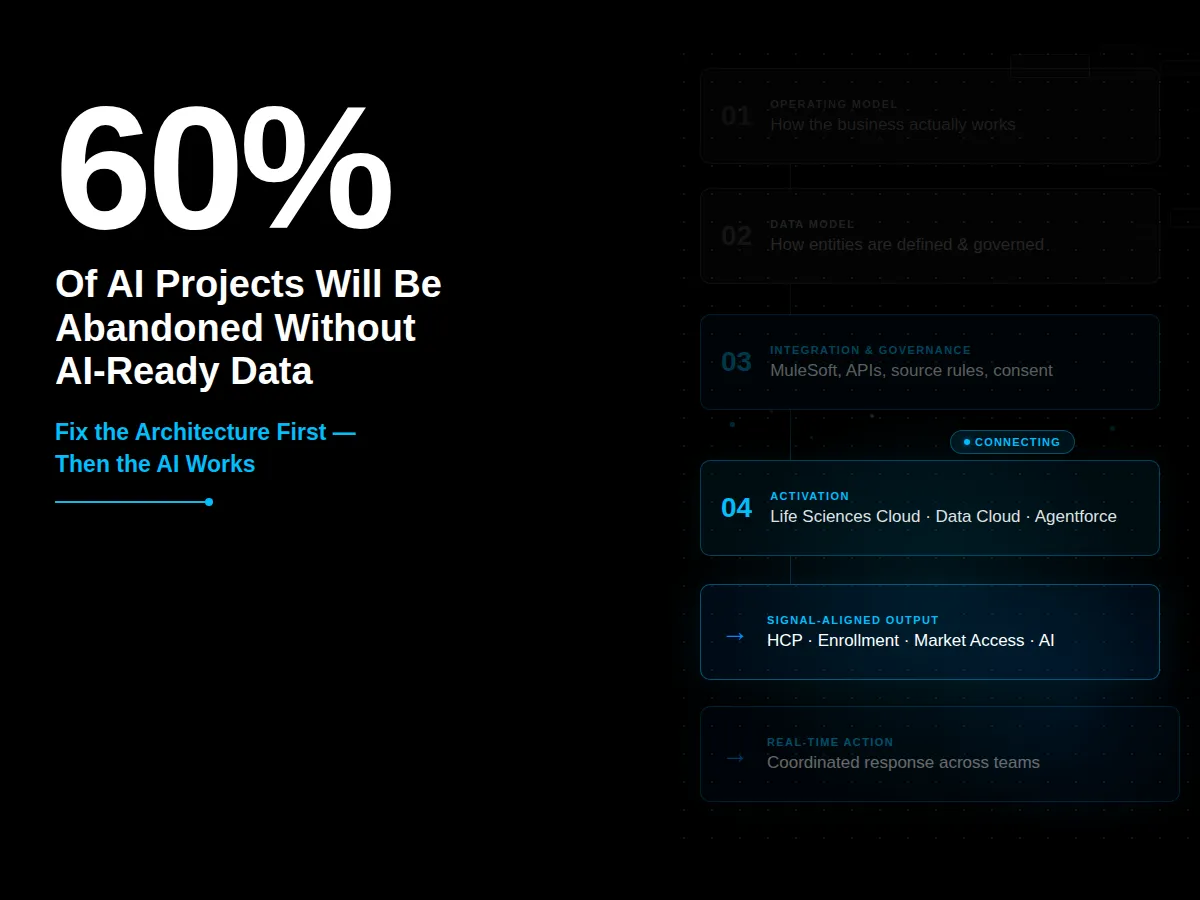
Gartner found that 63% of organizations either don’t have or aren’t sure they have the right data management practices to support AI. Gartner also predicts that through 2026, 60% of AI projects lacking AI-ready data will be abandoned. The tools aren’t the bottleneck. The architecture underneath them is. (Gartner, February 2025)
This article introduces CI Digital’s six-part series on building a connected pharma enterprise on Salesforce. Each article in the series covers one functional domain: HCP data architecture, patient enrollment orchestration, market access intelligence, signal-aligned architecture design, and HCP data fragmentation. This piece gives you the framework that ties them together.
What does “connected” actually mean for a pharma data environment?
Connected doesn’t mean centralized. Pharma organizations don’t need one system that holds everything. What “connected” means is that the systems you already run share identity, context, and signal in a way that produces consistent, actionable output.
A provider record in your CRM should reflect the same HCP as the one in your claims data and your speaker bureau system. An enrollment case should move through your patient services workflow with payer data, benefit investigation results, and specialty pharmacy status all visible in one place. A formulary change from a payer should surface to field teams, market access, and patient services at the same time, not in three separate reports three weeks later.
That’s connectivity in practice: not a single database, but a shared understanding of who the provider is, where the patient case stands, and what the access environment looks like. Salesforce Health Cloud was built to make exactly this possible for life sciences teams, but getting there requires more than a platform purchase.
Why do most pharma data environments stay fragmented?
The fragmentation usually traces to a structural decision made years ago: data problems got solved application by application instead of architecturally. A campaign needed a clean HCP list, so someone cleaned it for the campaign. A territory realignment needed accurate affiliations, so operations pulled and fixed the data for the alignment. None of those fixes addressed how provider identity, patient records, and payer data get defined, governed, and maintained across all the systems that use them.
McKinsey’s 2025 State of AI report found that while 88% of organizations use AI in at least one business function, only about one-third have scaled it enterprise-wide. In pharma, that piloting problem almost always traces to the same root cause: the data foundation wasn’t ready. AI surfaces fragmentation in ways that reporting never did, because AI needs consistent, governed, connected data to produce reliable output. (McKinsey, State of AI 2025, November 2025)
What does a connected Salesforce pharma architecture look like in practice?
The architecture has four layers. They’re not sequential in the sense that you finish one and start the next. But they’re foundational: each one depends on the ones below it.
The first layer is the operating model. Before any technology decision, you need to understand how the business actually works: who owns the patient journey, who manages provider engagement, who owns market access decisions, and where those functions hand off to each other. Technology recommendations that don’t reflect the operating model fail at adoption, not at implementation.
The second layer is the data model. How are patients, providers, payers, plans, products, cases, consents, and enrollments represented across your systems? Which system is authoritative for provider affiliations? How do you handle a provider who appears in five systems with five slightly different records? Getting this layer right is what separates pharma teams that can act on AI insights from those that can’t.
The third layer is integration and governance. Which systems are authoritative for which data fields? What consent, audit, and compliance controls apply? MuleSoft sits here, managing the communication between Salesforce and the external platforms your operation depends on: payer APIs, specialty pharmacy systems, EHRs, hub service platforms, and third-party data providers. This layer also defines the rules for data conflicts: which source wins for a given field, and who resolves exceptions.
The fourth layer is activation. Salesforce Life Sciences Cloud, Data Cloud, and Agentforce sit here. This is where unified provider identity gets used to drive segmentation, where enrollment status triggers the right workflow, and where a formulary change reaches field teams, patient services, and medical affairs automatically. The activation layer produces the business value. It only works when the first three layers are in place.
What are the five functional domains this series covers?
Each article in this series addresses one specific part of the architecture where pharma organizations consistently run into problems.
The HCP data piece covers what a real Provider 360 requires architecturally, and why a CRM doesn’t give you one. A Provider 360 requires canonical identity, data provenance, survivorship rules, and activation. Most organizations have at most one of those four things.
The patient enrollment piece covers why enrollment stalls in the handoffs, not the forms. Orchestration manages the full journey across intake, benefit investigation, prior authorization, specialty pharmacy coordination, and status communication. Automation speeds up individual steps. Orchestration manages the whole process.
The market access piece covers the difference between a reporting system and an activation system. Most pharma teams have dashboards. Very few have the architecture to detect a formulary change and coordinate a response across field, medical, and patient services in real time.
The signal-aligned architecture piece covers Jeff Sumption’s diagnostic framework: operating model first, data model second, integration and governance third. Only then does it make sense to select Salesforce configuration, Life Sciences Cloud capabilities, Data Cloud, or automation tooling.
The HCP data fragmentation piece explains why the same provider appears as five different records, why repeated data cleaning doesn’t solve it, and what Salesforce Data Cloud does differently at the identity layer.
Where does CI Digital fit into this?
CI Digital implements Salesforce Life Sciences Cloud, Data Cloud, and MuleSoft for pharma and life sciences organizations. The work Jeff Sumption describes in this series reflects what CI Digital sees on actual implementations: the operating model misalignments, the data model gaps, the integration sprawl, and the activation failures that happen when the foundation isn’t right.
If your organization is evaluating Salesforce Life Sciences Cloud, migrating from Veeva, or trying to connect a fragmented pharma stack, the five articles in this series give you a practitioner-level framework for what’s required. Talk to our Salesforce team about where to start.
Frequently asked questions
What is a connected pharma architecture on Salesforce?
A connected pharma architecture on Salesforce means your HCP, patient, payer, and enrollment data share a unified identity and governance model, so the business can act on signals in real time instead of reconciling reports after the fact. It typically combines Salesforce Life Sciences Cloud for workflow orchestration, Data Cloud for identity resolution and segmentation, and MuleSoft for integrating external systems like payer APIs, specialty pharmacies, and EHRs.
Why do pharma data environments stay fragmented even after CRM implementation?
CRM implementation solves the workflow layer, not the data foundation layer. Fragmentation in pharma traces to decades of application-specific data cleaning: teams fix HCP records for a campaign or a territory alignment, but they don’t solve how provider identity, patient records, and payer data get defined and governed across all systems. The CRM inherits the fragmentation rather than resolving it.
What is Salesforce Life Sciences Cloud and how does it differ from Health Cloud?
Salesforce Life Sciences Cloud is Salesforce’s purpose-built platform for pharma and medical technology organizations, generally available since October 2025. It includes capabilities for patient services, HCP engagement, clinical trial management, and enrollment orchestration on a HIPAA-ready, GxP-compliant foundation. Health Cloud is Salesforce’s broader healthcare platform. Life Sciences Cloud addresses the specific compliance and engagement requirements of pharma and medtech.
What does Salesforce Data Cloud do for pharma teams specifically?
Data Cloud lets pharma teams unify HCP and patient data across systems without forcing every source system to become the system of record for everything. It handles identity resolution, segmentation, calculated insights, and activation across Salesforce clouds and connected external systems. For pharma, this means connecting signals from claims, CRM interactions, payer data, and enrollment workflows into one data layer the business can act on.
How does MuleSoft connect to Salesforce Life Sciences Cloud for pharma?
MuleSoft connects Salesforce Life Sciences Cloud to the external systems that pharma workflows depend on: payer APIs, electronic prior authorization vendors, specialty pharmacy systems, EHRs, hub service platforms, and benefits verification tools. In a mature architecture, Salesforce owns the workflow orchestration while MuleSoft manages the system-to-system data flows and API governance that make the integration layer scalable and auditable.
Author

Jeff Sumption

Share this article
Subject Matter Expert
Jeff Sumption
Salesforce Solution Architect
Speak With Our Team
Share this article